
-

There is no road map when the diagnosis ...
-
The feeding tube and palliative care
-

Before you order a (swallow) test, ask �...
-

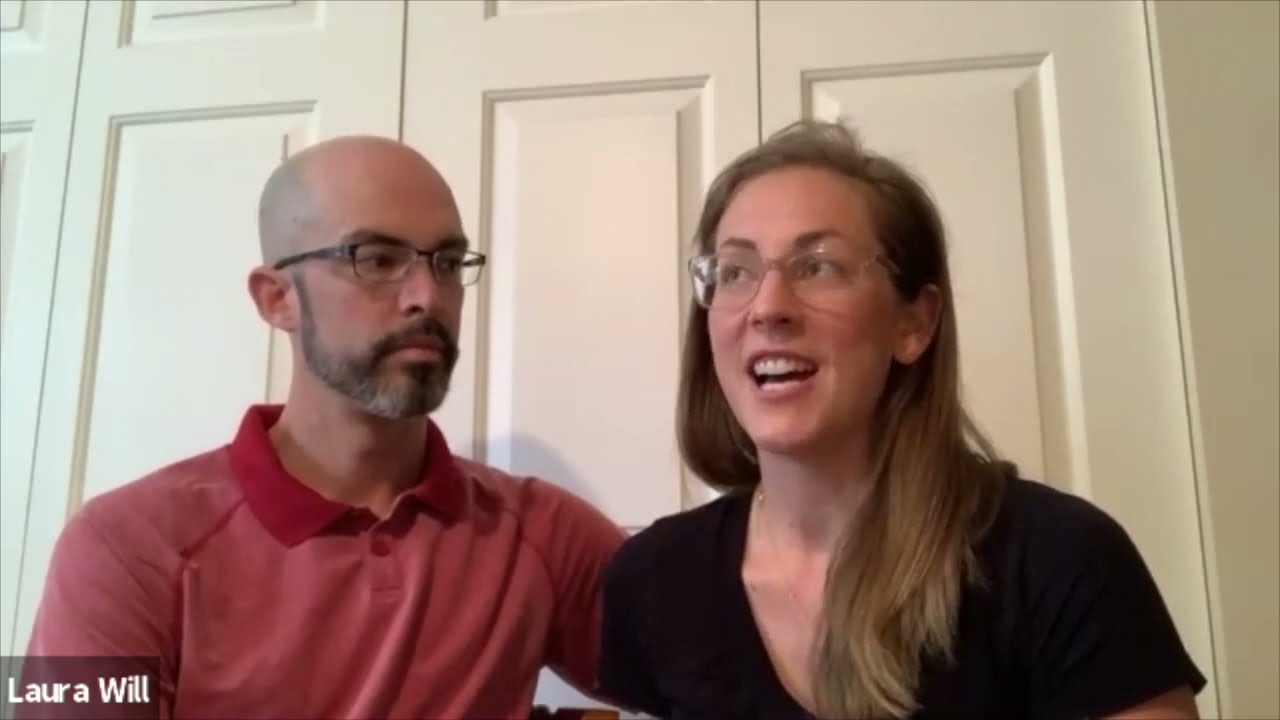
A Mom on deciding about a feeding tube f...
-

I had never met anyone whose child had a...
-

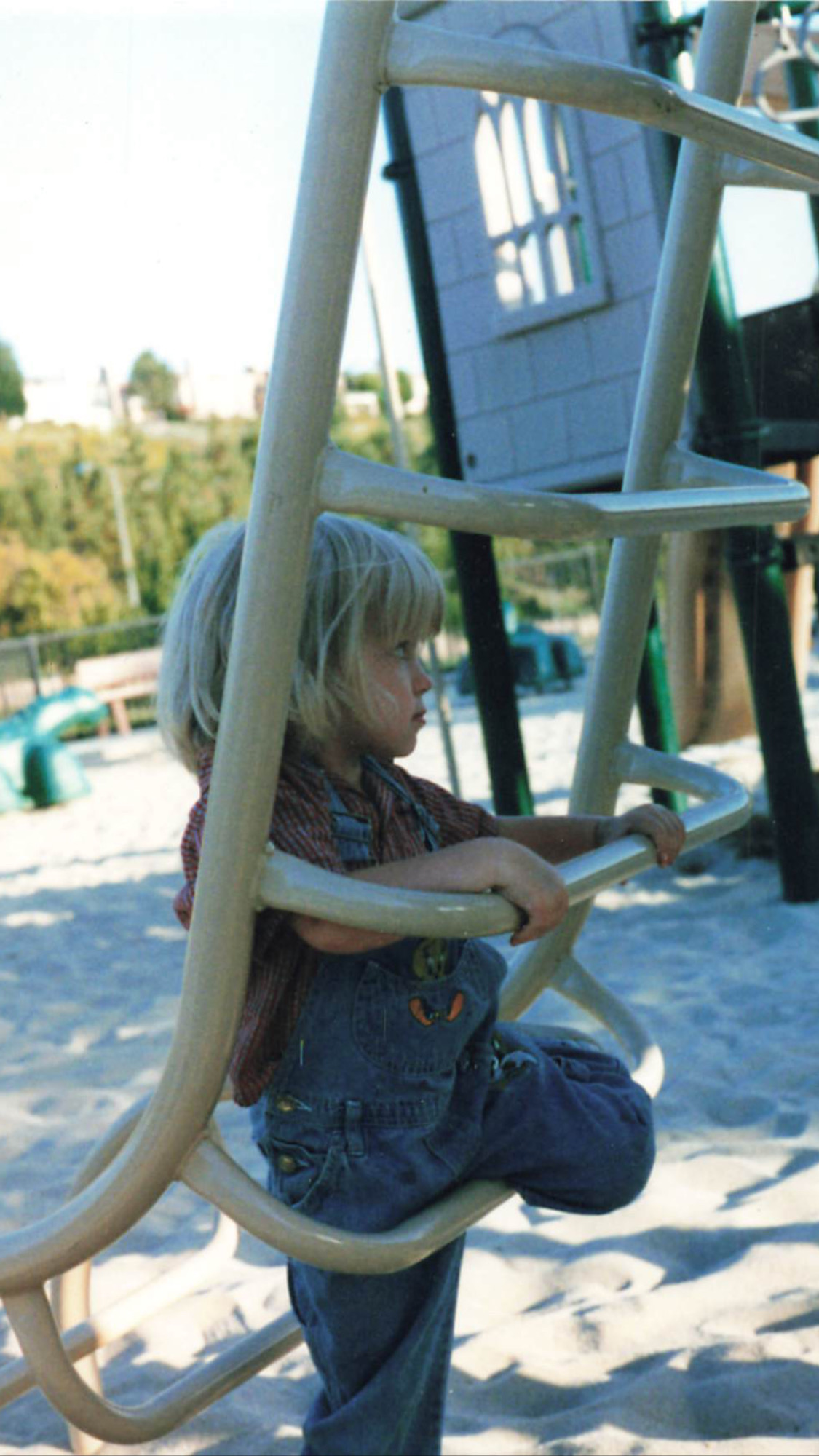
I was devastated — Suddenly my bab...
-

A feeding tube: Other parents gave us pe...
-
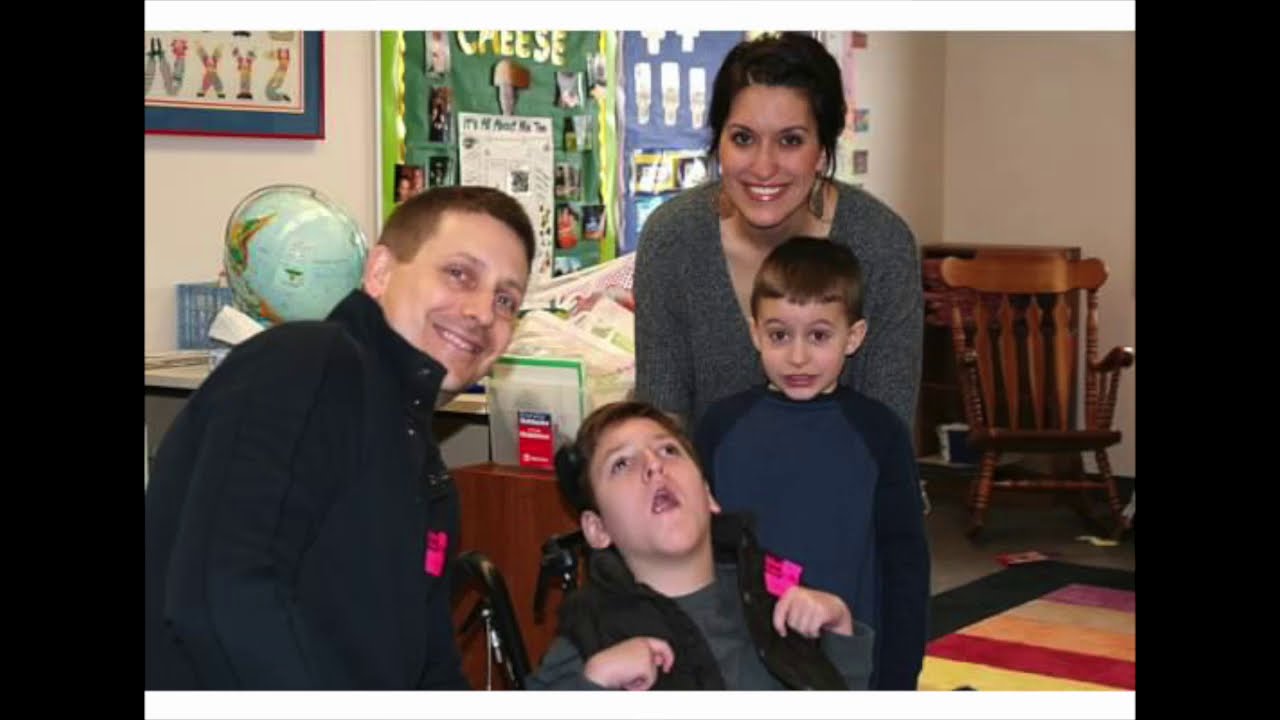
Parenting a Medically Complex Child: Dec...
-

The doctor explained: not doing a feedin...
-

We were actively protecting her from thi...
-

The Feeding Tube is a difficult decision...
-

How we thought about a feeding tube or n...
SHARE

Videos
SHARE
Theme: Feeding Tubes
There is no road map when the diagnosis is so rare.
Page: 1 of 2
There is no road map when the diagnosis is so rare.
SHARE
1 / 16
Related Resources
-
 PostDid I Play God?
PostDid I Play God? -
 PostNavigating Decisions Surrounding Feeding Intolerance
PostNavigating Decisions Surrounding Feeding Intolerance -
 PostHow Food Brought Joy to My Daughter Even When She Could No Longer Eat
PostHow Food Brought Joy to My Daughter Even When She Could No Longer Eat -
 EventWhen it’s harder than it should be: Navigating the emotional toll of your child’s feeding challenges
EventWhen it’s harder than it should be: Navigating the emotional toll of your child’s feeding challenges -
 GuideWhat is Tube Feeding?
GuideWhat is Tube Feeding? -
 PostA Guide to Understanding Your Child's Nutritional Needs Throughout Illness and at End of Life
PostA Guide to Understanding Your Child's Nutritional Needs Throughout Illness and at End of Life