
-

A diagnosis of Krabbe; and the medical t...
-

We were so caught up in having a new bab...
-

Adding Hospice to the Care Team
-

What does a “good day” look like? Em...
-

This is How We Live: This Thing Called B...
-

Palliative care helps parents pause and ...
-
Problems of the CNS: Is this a new acute...
-
Intractable problems and a new Baseline:...
-
The Conversation and Advance Care Planni...
-

Always give them a sense of what’s goi...

Videos
SHARE
Theme: Baseline
A diagnosis of Krabbe; and the medical team getting to meet him before his condition progressed.
A diagnosis of Krabbe; and the medical team getting to meet him before his condition progressed.
SHARE
1 / 10
Related Resources
-
 PostLearning Her Again; A Mother’s Understanding of Baseline
PostLearning Her Again; A Mother’s Understanding of Baseline -
 PostDid I Play God?
PostDid I Play God? -
 PostNavigating therapies when your child has a rare and fatal disease
PostNavigating therapies when your child has a rare and fatal disease -
 PostYour Child’s Baseline and Time Under Tension
PostYour Child’s Baseline and Time Under Tension -
 PostA Parent's Narrative of Their Child is the Baseline
PostA Parent's Narrative of Their Child is the Baseline -
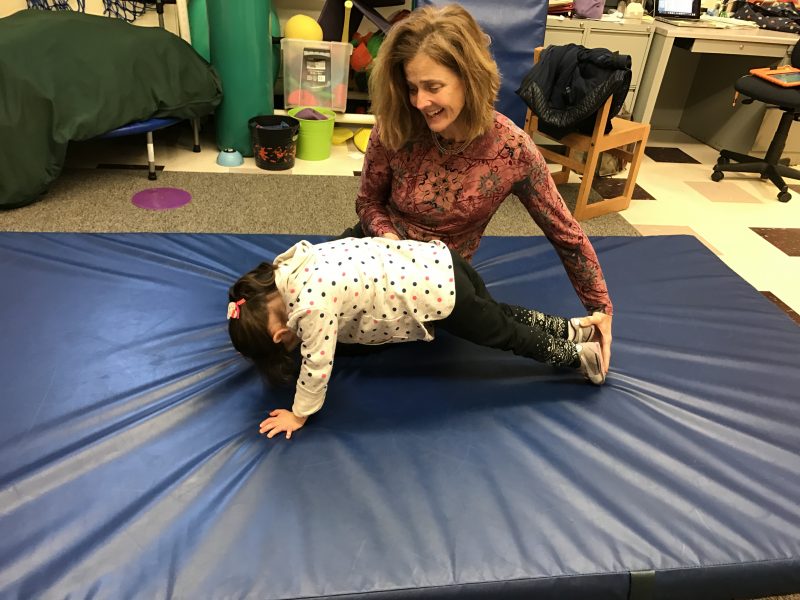 PostA Physical Therapist’s Perspective on Shifting Baseline
PostA Physical Therapist’s Perspective on Shifting Baseline