-
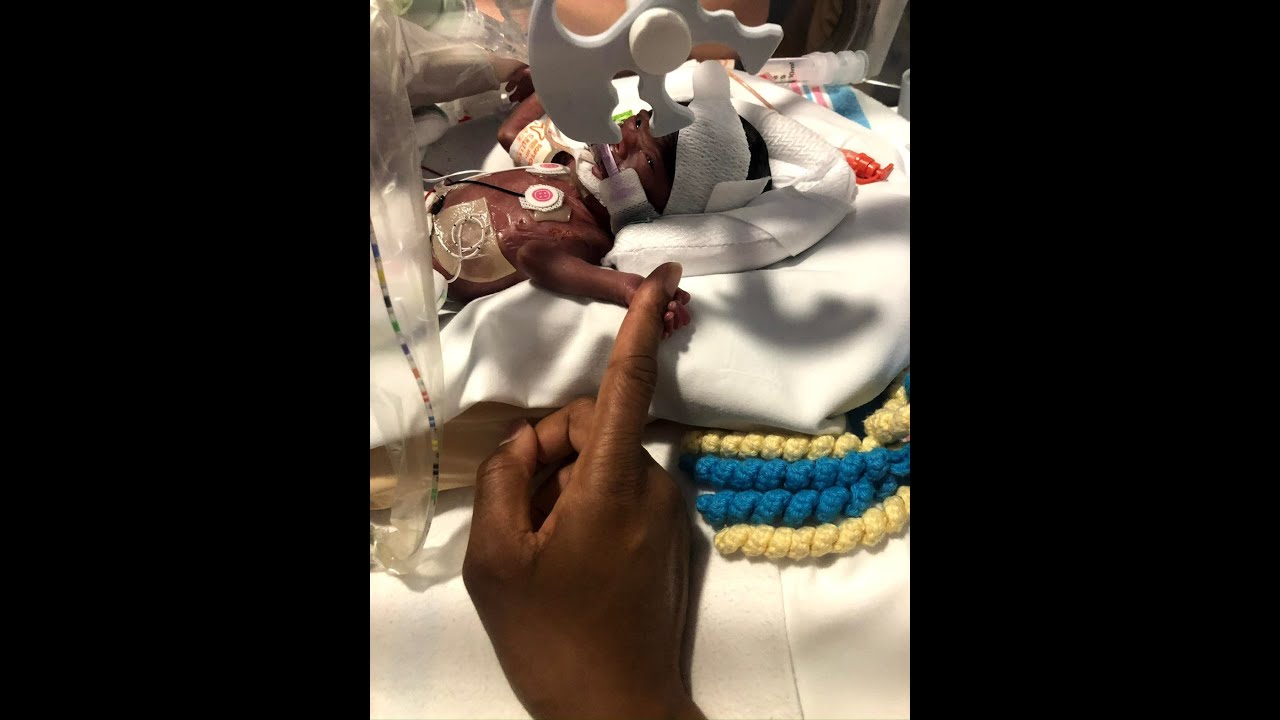
Decision-making in the NICU: When the mo...
-

Wondering if your child is going to be t...
-

Grief: “Have grace with your spouse.�...
-

A parenting journey like this “tests a...
-
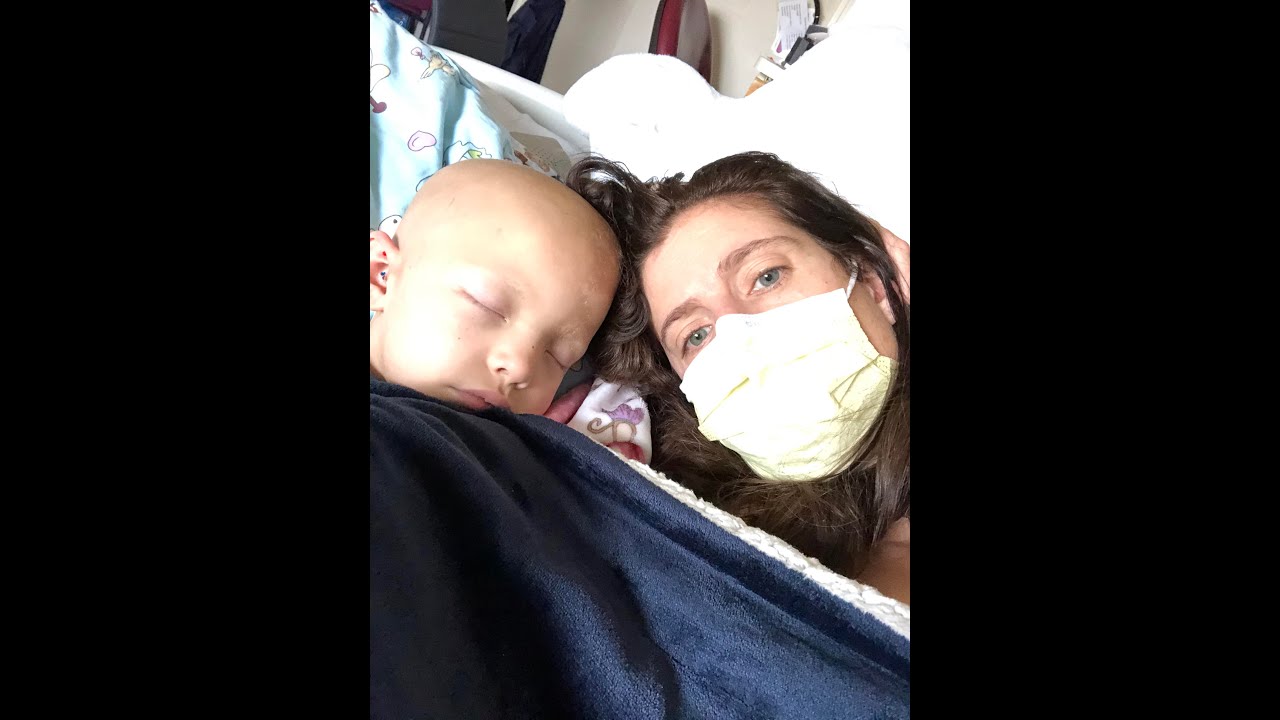
When only one parent is in the hospital:...
-

I wanted to be strong for her but there ...
-

A dad reflects on living in the hospital...
-

It’s important to remind ourselves we�...
-

Marriage: Finding touchstones for the re...
-

If we hadn’t gotten married for the ri...
-

Spinal Fusion Surgery: Creating a space ...
-

As a parent, you do what you have to do....
SHARE

Videos
SHARE
Theme: Partnership and Marriage
Decision-making in the NICU: When the mom and dad are thinking at different scales of time
Page: 1 of 4
Decision-making in the NICU: When the mom and dad are thinking at different scales of time
SHARE